ORIGINAL RESEARCH |
https://doi.org/10.5005/jp-journals-10024-3126 |
Evaluation of Orthodontic Mini-implant-anchored en masse Retraction of Maxillary Anterior Teeth with Reduced Bone Support: A Prospective Finite Element Analysis Study
1–5Department of Orthodontics and Dentofacial Orthopedics, Faculty of Dental Sciences, Ramaiah University of Applied Sciences, Bengaluru, Karnataka, India
Corresponding Author: Ashok Kumar, Department of Orthodontics and Dentofacial Orthopedics, Faculty of Dental Sciences, Ramaiah University of Applied Sciences, Bengaluru, Karnataka, India, Phone: +91 9943168569, e-mail: ashokmd5597@gmail.com
How to cite this article: Sahasrabudhe S, Sunil Kumar M, Khan IS, et al. Evaluation of Orthodontic Mini-implant-anchored en masse Retraction of Maxillary Anterior Teeth with Reduced Bone Support: A Prospective Finite Element Analysis Study. J Contemp Dent Pract 2021;22(7):833–839.
Source of support: Nil
Conflict of interest: None
ABSTRACT
Aim: The purpose of this study was to evaluate force systems to bring about the en masse retraction of maxillary anterior teeth having reduced bone levels using finite element analysis.
Materials and methods: This is a prospective study. Three-dimensional finite element models of maxillary dentition having normal alveolar bone level and 2, 4, and 6 mm bone loss with first premolar extraction were constructed from a spiral CT scan of a skull. Archwire and brackets were modeled on the facial surfaces of teeth. Retraction force of 175 gm was applied from an orthodontic mini-implant placed bilaterally between the second premolar and first molar and 12 mm above plane of the archwire to anterior retraction hook (ARH) fixed at two heights of 6 and 10 mm above the archwire.
Results: Maximum displacement and periodontal ligament (PDL) stress were calculated for different combinations of bone levels and ARH. As the bone loss increased, the tipping tendency, amount of intrusion, and maximum von Mises stress in PDL also increased, showing a direct correlation.
Conclusion: To minimize tipping and PDL stress, the height of ARH should be increased in alveolar bone loss conditions to allow retraction force to pass through or even above the center of resistance of anterior teeth. Even then, pure bodily retraction may not be achieved, but tipping tendency can be reduced. Nevertheless, it may not be suitable to increase ARH beyond a limit owing to chances of irritation to the vestibular mucosa. Alternative methods should be contemplated to reduce the tipping behavior.
Clinical significance: The alternative is to apply a lighter retraction force to reduce lingual tipping. A higher counter-moment in the archwire or bracket can also be incorporated.
Keywords: Alveolar bone loss, Anterior retraction hook, Finite element analysis, Orthodontic mini-implant.
INTRODUCTION
In contemporary orthodontic practice, clinicians are witnessing an upsurge in the number of adult patients with proclined maxillary anterior teeth complicated by alveolar bone loss. In patients with active periodontal disease, orthodontic treatment is contraindicated because it may accelerate tissue breakdown. However, it is clearly indicated in cases where the disease is well under control, even in presence of bone loss and gingival recession. It is also believed that with the orthodontic treatment, the patient may not experience additional loss of bone support.1,2
A common sequel of periodontal disease is alveolar bone loss which in the long term, increases masticatory load on the anterior teeth leading to their migration, extrusion and further protrusion.3 A common treatment approach for such patients with periodontal compromise is first premolar extraction with space closure requiring maximum anchorage mechanics. The use of orthodontic mini-implant (OMI) for reinforcement of anchorage has been on the rise in recent years, especially for space closure in sliding mechanics. Position of OMI is preferred in apical portion, between the second premolar and first molar or first and second molar roots to direct the force vector toward the center of resistance (CoR) of teeth for effective retraction.
The balance between the location of the CoR and the effects of varying level of retraction force on the anterior segment is known to produce desired moment to force ratio (M/F) for controlled tooth movement.4 Also periodontally compromised malocclusion with bone loss poses a greater challenge to the orthodontist as the alveolar bone loss results in the shift of CoR apically increasing the moment generated by the same force. In order to achieve controlled retraction of anterior teeth in such cases, certain modifications in the force systems are necessary.5
Orthodontic mechanics by and large is extrusive in nature. A key in the treatment of periodontally compromised teeth is to prevent their further extrusion or achieve true intrusion. Good control is required not only in the anteroposterior direction (during retraction) but also in the vertical direction. Mini-implants are a good choice for intruding teeth because they make it possible to apply light continuous forces of known magnitudes without producing any reactionary reciprocal side effect on posterior teeth, which could help reduce potential apical root resorption often associated with intrusive movements.6 This can be beneficial especially in the orthodontic treatment of teeth with periodontal bone loss. However, the use of OMI to achieve effective en masse retraction of incisors in periodontally compromised patients has not been addressed adequately in the literature.
The aim of this study was to evaluate the force systems which bring about retraction and intrusion of anterior maxillary dentition with normal marginal bone level and with varying alveolar bone loss conditions using OMI.
MATERIALS AND METHODS
Generation of 3D Finite Element Model
This is a prospective study. A spiral CT scan (X-force/SH spiral CT scan machine) of a skull was used as a basis. The CT images with a slice thickness of 0.25 mm were extracted as digital imaging and communication in medicine data and exported to 3D image processing software (Mimics 10.02, Materialize Software, Leuven, Belgium) and only the region of interest of the study (maxilla) was selected. Once the surface model was obtained, it was exported to finite element modeling tool HYPERMESH version 10.0 (Altair Engineering, Milwaukee, Wisconsin).
Models of the maxillary dentition with bilateral first premolar extractions with normal alveolar bone level and with 2, 4, and 6 mm marginal bone loss in the anterior region (from distal surfaces of canine to canine) were simulated and converted into a finite element model.
The periodontal ligament (PDL) was constructed with uniform thickness of 0.25 mm. The alveolar bone crest was simulated to follow the curve of the cementoenamel junction (CEJ) in the model with no bone loss. On the contrary, the alveolar bone crest was constructed 2, 4, and 6 mm apically from canine to canine (from the distal surface of canine) in the bone loss models still following the curvature of CEJ. All the models of the maxilla were fixed in all directions and discretized in x, y, and z axes. The x axis was fixed in the mediolateral direction, the y axis was fixed in the anteroposterior direction, and the z axis was fixed in the superoinferior (vertical) direction (Fig. 1).
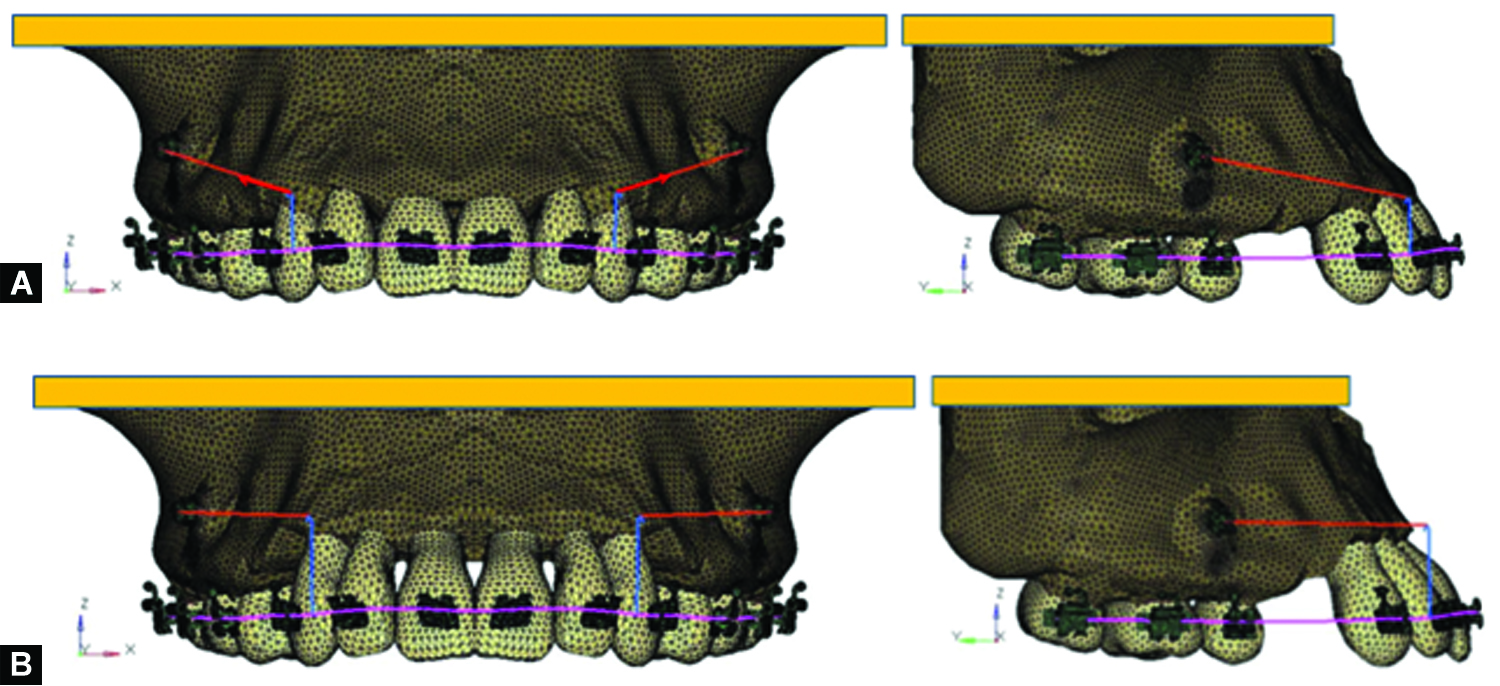
Figs 1A and B: FEA models of maxillary dentition with OMI placed at 12 mm with variable ARH. (A) Group 1A, no bone loss, ARH 6 mm; (B) Group 4H, 6 mm bone loss, ARH 10 mm. *Purple line represents archwire, blue vertical line between lateral incisor and canine represents ARH, and red line represents line of force application
Assigning Material Properties
The material properties assigned were the Young’s modulus (modulus of elasticity) and the Poisson’s ratio (Table 1). The bone element and PDL were assumed to be isotropic and homogeneous. The archwire was modeled by beam four elements with a cross-section of 0.019 × 0.025 inch stainless steel wire with anterior retraction hook (ARH) of 0.05 inch stainless steel wire fixed between lateral incisor and canine. Brackets with 0.022 × 0.028 inch slot were modeled. A titanium mini-implant of 1.6 mm diameter and 8 mm length was placed midway mesiodistally between the maxillary second premolar and first molar roots, in the alveolar bone, 12 mm above the plane of the archwire. Two heights of ARH, i.e., 6 and 10 mm were selected on the archwire between lateral incisor and canine. The placement of an ARH between the lateral incisor and canine enables the orthodontist to gain better control of the anterior teeth in sliding mechanics.7
| Material | Young’s modulus | Poison’s ratio |
|---|---|---|
| Teeth | 2E6 | 0.3 |
| PDL | 5.0 | 0.3 |
| Alveolar bone | 2E5 | 0.3 |
| Stainless steel | 2E7 | 0.3 |
| Titanium | 110E3* | 0.3 |
Execution of Analysis
The boundary conditions were defined for all models. The nodes attached to the area of the outer surface of the bone were fixed in all directions to avoid free movement of the tooth. Free axial rotation movement of the archwire in the brackets was allowed, while friction between the archwire and brackets along the axial direction was not taken into consideration. Using ANSYS software version 12.1 (ANSYS Inc., Canonsburg, Pennsylvania, USA), analysis was carried out. A retraction force of 175 gm was applied on the ARH bilaterally from the mini-implants. The angle of displacement of central incisor, lateral incisor, and canine, the amount of intrusion of crown and root tip for each tooth in all the groups and von Mises stress in PDL were recorded, studied on mesh graphs, and were represented on the color band. The red color in the scale showed the maximum von Mises stress with the blue color indicated the minimum stress. The force magnitude was also resolved in all the three axes (Table 2).
| Force (gm) | ARH 6 mm | ARH 10 mm |
|---|---|---|
| Fx | 89.8 | 91 |
| Fy | 147.3 | 149.4 |
| Fz | 29.4 | 25 |
| Fz/Fx (%) | 19.96 | 16.7 |
RESULTS
The results obtained from the finite element analysis (FEA) were divided into four groups depending on the amount of bone loss constructed in the models, and each group was further categorized into two subgroups of 6 and 10 mm ARH heights (Table 3). Comparisons were made among the subgroups within a group (intragroup comparison), between different groups (intergroup comparison), and also between two ARH conditions in the study.
| Bone level | Group | Subgroup | ARH height (in mm) |
|---|---|---|---|
| Normal | 1 | A | 6 |
| B | 10 | ||
| 2 mm bone loss | 2 | C | 6 |
| D | 10 | ||
| 4 mm bone loss | 3 | E | 6 |
| F | 10 | ||
| 6 mm bone loss | 4 | G | 6 |
| H | 10 |
When the retraction force was applied to the six maxillary anterior teeth with miniscrews and retraction hooks in different positions, the central incisor, lateral incisor, and canine showed intrusion accompanied by lingual tipping movement (Fig. 2). The degree of tipping varied depending on the locations of the hooks and the degree of alveolar bone loss because of changes in the relative force magnitude and direction.8 Within each group the tipping angle, the amount of intrusion and the von Mises stress in PDL were higher for 6 mm ARH subgroups than for 10 mm ARH subgroups. This pattern was consistent for all the bone level groups. Lingual tipping of all anterior teeth occurred with maximum displacement at the lateral incisor crown level. Within each subgroup, tipping was the maximum for the canine followed by lateral incisor and was least in the central incisor. The tipping angle, the amount of intrusion, and von Mises stresses showed a tendency to increase with an increase in the alveolar bone loss (Table 4(I), (II), and (III), Figs 4 to 6). Maximum stress value was observed on the labiocervical third of the lateral incisor root area in groups 1, 2, and 3 and was seen on mesiocervical root of lateral incisor in group 4. Stress distribution was almost even in other areas. The least stress value was observed on central incisor roots (Fig. 3).
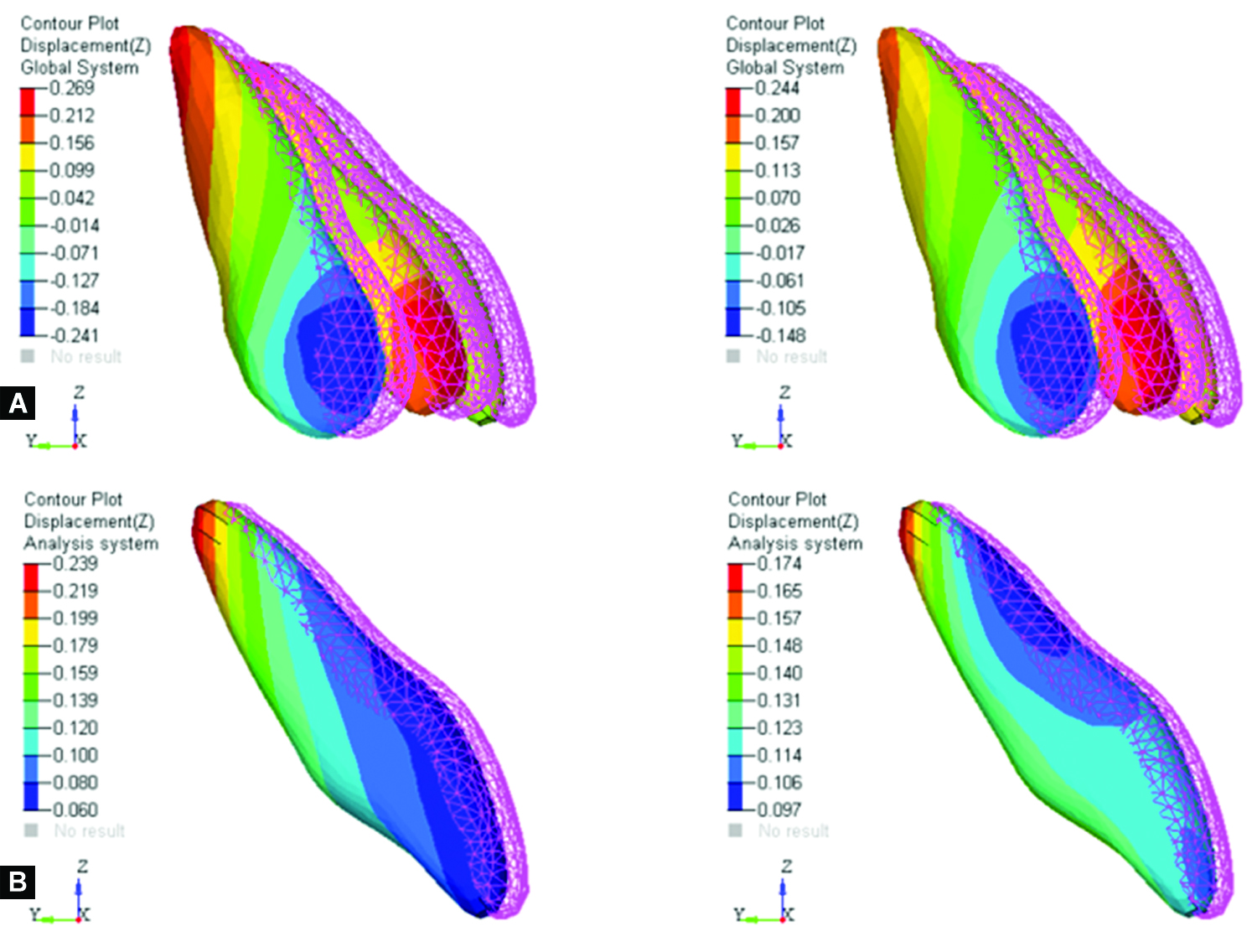
Figs 2A and B: Displacement contours of anterior teeth depicting their lingual tipping (I) and intrusion (II) in models with normal bone level (Groups 1A and 1B) and variable ARH. *(I) angle of tip for each anterior tooth, (II) amount of intrusion measured along the z axis. The pink mesh diagram indicates the original tooth position while the multicolored diagram indicates the final tooth position. The red two-way arrow in each central incisor diagram shows the tipping angle. The dotted black lines indicate the original and final axes of the tooth
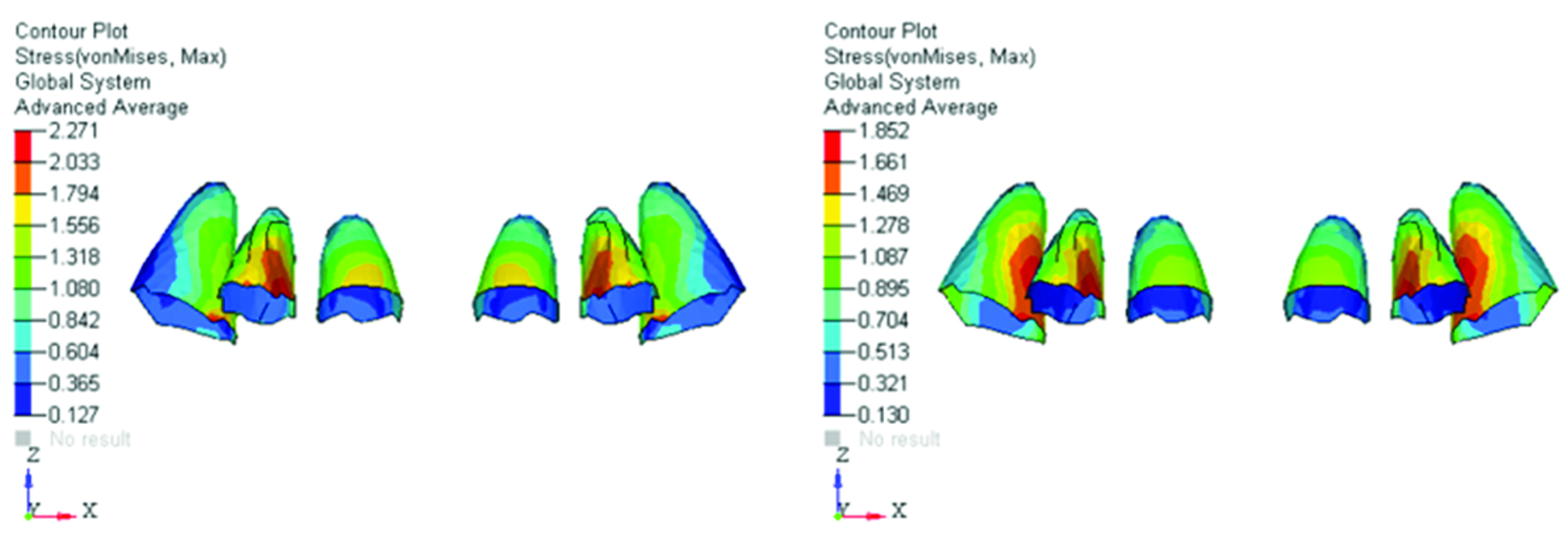
Fig. 3: Diagram showing color bands depicting von Mises stress levels in PDL of 6 mm bone loss models (Groups 4G and 4H) with variable ARH. *Red color indicates maximum stress whereas dark blue indicates minimum stress
| 6 mm ARH | 10 mm ARH | ||||||
|---|---|---|---|---|---|---|---|
| Bone loss (mm) | CI | LI | CN | CI | LI | CN | |
| (I) Tipping angle in degree (°) | |||||||
| 0 | 2.3 | 3.1 | 4.2 | 1.8 | 2.5 | 3.6 | |
| 2 | 3.1 | 4.5 | 5.6 | 2.5 | 3.9 | 4.8 | |
| 4 | 4.6 | 5.9 | 7.1 | 3.8 | 5.1 | 6.3 | |
| 6 | 6.2 | 7.5 | 8.6 | 5.4 | 6.3 | 7.5 | |
| *Tipping angle measured as the angle formed between long axes of original and final tooth positions along the y axis; CI, central incisor; LI, lateral incisor; CN, canine |
|||||||
| (II) Intrusion in mm along z axis | |||||||
| 0 | Crown | 0.100 | 0.208 | 0.078 | 0.097 | 0.165 | 0.036 |
| Root | 0.239 | 0.269 | 0.254 | 0.174 | 0.244 | 0.190 | |
| 2 | Crown | 0.071 | 0.184 | 0.143 | 0.100 | 0.163 | 0.067 |
| Root | 0.275 | 0.315 | 0.296 | 0.184 | 0.267 | 0.208 | |
| 4 | Crown | −0.021 | 0.187 | −0.159 | 0.128 | 0.205 | −0.095 |
| Root | 0.318 | 0.376 | 0.320 | 0.211 | 0.314 | 0.226 | |
| 6 | Crown | 0.005 | 0.218 | −0.064 | 0.204 | 0.263 | −0.072 |
| Root | 0.349 | 0.411 | 0.386 | 0.245 | 0.395 | 0.295 | |
| *Values with −sign indicate extrusion while values with no prefix sign are considered positive and for intrusion | |||||||
| (III) Maximum von Mises stress in PDL | |||||||
| Cervical | 0.157 | 1.031 | 1.031 | 0.118 | 0.692 | 0.431 | |
| 0 | Middle | 0.703 | 0.812 | 0.594 | 0.597 | 0.788 | 0.501 |
| Apical | 0.266 | 0.157 | 0.266 | 0.214 | 0.118 | 0.214 | |
| Cervical | 0.778 | 1.359 | 1.069 | 0.431 | 0.914 | 0.721 | |
| 2 | Middle | 1.069 | 0.923 | 0.633 | 0.624 | 0.817 | 0.624 |
| Apical | 0.342 | 0.488 | 0.342 | 0.238 | 0.238 | 0.238 | |
| Cervical | 1.013 | 1.599 | 1.004 | 0.705 | 1.221 | 1.393 | |
| 4 | Middle | 1.004 | 1.400 | 1.211 | 1.189 | 1.393 | 1.189 |
| Apical | 0.409 | 0.608 | 0.409 | 0.276 | 0.472 | 0.276 | |
| Cervical | 1.556 | 2.271 | 2.033 | 1.278 | 1.852 | 1.661 | |
| 6 | Middle | 1.080 | 1.794 | 1.318 | 1.469 | 1.661 | 1.469 |
| Apical | 0.604 | 0.842 | 0.604 | 0.321 | 0.704 | 0.513 | |

Fig. 4: Tipping angle variation for 6 mm ARH
In all the four models with varying bone levels and 6 mm ARH condition (groups 1A, 2C, 3E, and 4G), there was an increase in the tipping angle gradually with an increase in bone loss (Table 4(I), Fig. 4), with minimum in group 1A and maximum in group 4G. The intrusion values increased in a similar pattern, increasing though slightly, from group 1A to 4G successively (Table 4(II)). Maximum von Mises stresses in PDL showed a similar direct relation with the amount of bone loss (Table 4(III), Fig. 6).
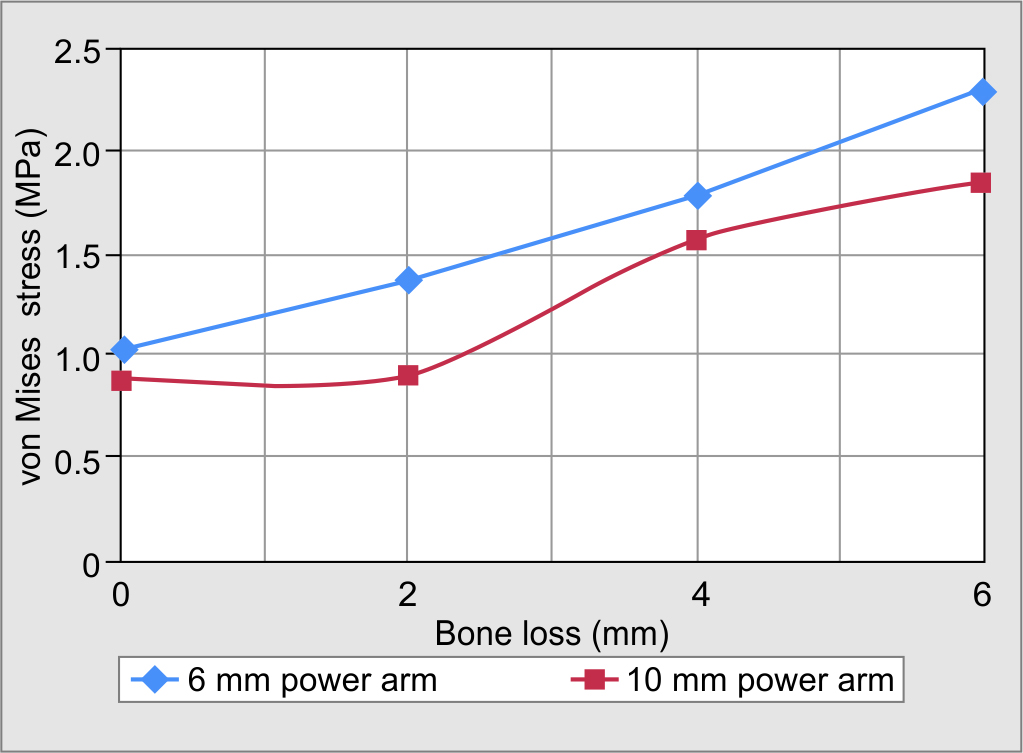
Fig. 6: Variation of maximum von Mises stress generated in the PDL
In all the four models with varying bone levels with 10 mm ARH condition (1B, 2D, 3F, and 4H), an increase in the tipping angle gradually from group 1B to 4H was noted (Table 4(I), Fig. 5).
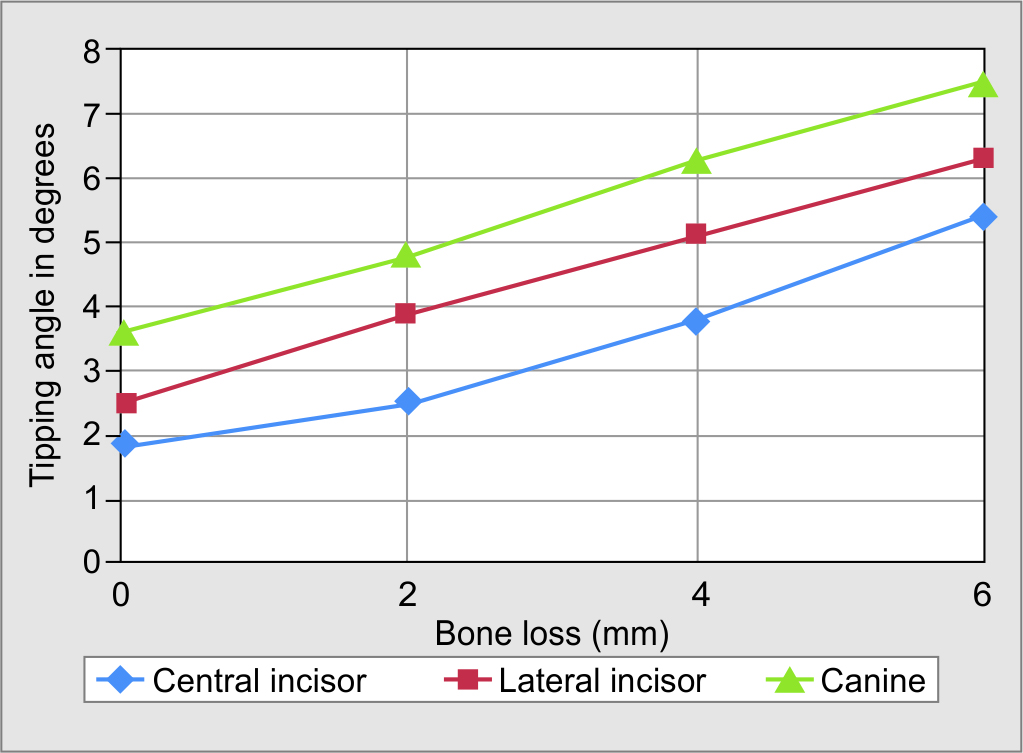
Fig. 5: Tipping angle variation for 10 mm ARH
The intrusion values showed a similar pattern, increasing though slightly, from group 1B to 4H successively (Table 4(II)). The stress value was least for group 1A increasing through group 2C and 3E reaching the maximum in group 4G (Table 4(III), Fig. 6).
DISCUSSION
As the CoR of a tooth or group of teeth shifted apically with loss of alveolar bone, the tipping angle increased gradually with an increase in bone loss. This can be attributed to the increase in the moment arm and subsequent increase in the moment generated by the retraction force. This finding was in accordance with previous studies.5,9,10 Also because the retraction force was expected to pass below the CoR of the anterior dentition, the moment generated was clockwise.
The increase in amount of intrusion with increased bone loss can be attributed to fact that the retraction force used in all the groups was the same, whereas the PDL area on which it was applied decreased with bone loss resulting in more force applied per unit area of PDL in bone loss groups.
As the amount of alveolar bone support reduced, there was an increase in the amount of von Mises stress generated in the PDL. This finding was in congruence with previously conducted FEA studies.11–14
Similarly, to the above case, the lingual tipping of the anterior teeth increased with increase in bone loss in 10 mm ARH models. The shift of CoR of a tooth or group of teeth apically with loss of alveolar bone resulted in an increase of the tipping angle due to an increase in the moment arm. In these models, the resultant force was expected to pass at least through or above the CoR of the anterior dentition; and the moment generated due to retraction force was expected to be counterclockwise. But the labial tipping of the anterior teeth beyond their original long axes was not seen.
As with 6 mm ARH condition, with 10 mm ARH situation, there was a definite increase in the amount of intrusion of anterior teeth with increasing bone loss. The reason for the same is mentioned before.
The von Mises stresses in PDL observed in these four groups showed a similar direct relation, i.e., an increase in stress value with the increase in the amount of bone loss. It can be concluded from the above data, that as the amount of alveolar bone support reduced, there was increase in the amount of stress generated in the PDL.
Difference was observed in the tooth movement with different ARH heights (6 and 10 mm) and the von Mises stresses generated in the PDL. For the same amount of bone loss in all the four groups, the amount of clockwise (lingual) tipping was more with 6 mm ARH than with 10 mm ARH. A finite element study by Sung et al. showed similar results where; as the height of the ARH increased, the lingual tipping of incisors reduced.15
Also, the amount of intrusion was more in the models with 6 mm than with 10 mm ARH (Table 4(II)). Congruent results were found in the study by Sung et al., in which, when the ARH increased, the amount of intrusion decreased gradually.15 The vertical component of the retraction force was slightly more with 6 mm than 10 mm ARH (Table 2) which justified more intrusive force for 6 mm ARH models compared to 10 mm ARH models, and this held true for all the groups.
The stresses generated in PDL decreased with 10 mm ARH compared to 6 mm ARH conditions in all four groups (Table 4(III), Fig. 6). This finding was in agreement with another study done by Ammar et al. which showed a reduction of PDL stress magnitudes with increasing hook length. This can be attributable to the shorter moment or the power arm from the tooth’s center of rotation to the point of force application, resulting in lower bending stress.16
Orthodontic treatment of periodontally compromised adults having procumbent incisors with alveolar bone loss has been a clinical challenge that demands premolar extraction and space closure requiring good anchorage control. During retraction using sliding mechanics, heights of retraction forces can be manipulated by soldering different lengths of retraction hooks to the archwire. Therefore, the force system for the desired tooth movement can be simply applied.17 Nonetheless, clinicians tend to simply guess the height. This is because the guidelines for optimum mechanical parameters for the control of the anterior teeth in space closure with sliding mechanics are not yet established.18
Mini-implant-anchored sliding mechanics provides better anchorage control for bodily retraction of maxillary anteriors at times with slight intrusion by making the force pass near the CoR. The vertical positioning of OMI dictates the force direction so that the retraction of the anterior teeth can be controlled. The second factor influencing the force direction is the vertical position of the ARH. Use of short ARH increases the vertical component and decreases the horizontal component of the force and vice versa. When bodily movement is required, the retraction force should be applied as apical as possible using high ARH, making the force vector pass as close to CoR as possible.19
Finite element method is a powerful computer simulation tool for solving complex stress-strain problems and offering accurate modeling of teeth and surrounding structures with complicated geometry. It is very useful to analyze orthodontic forces, initial reaction of teeth, PDL and alveolar bone to orthodontic forces, the stress-strain and displacement qualitatively and quantitatively.15
It can be concluded from the results of this study that the best combination of the OMI height and the ARH height to bring about near bodily tooth movement was 12 and 10 mm, respectively, in all the groups with varying bone loss. Even then, a pure bodily retraction of anterior teeth could not be achieved but the tipping tendency was reduced. On the contrary, more intrusion could be achieved using 12 mm OMI height and 6 mm ARH height in all the groups. Forces applied coronal to the CoR resulted in the generation of the clockwise moment, causing lingual tipping of anterior teeth.
In a case series done by Park and Kwon, it was concluded that for bodily retraction of the anterior teeth with a slight intrusion, the ideal position of the OMI was 8 to 10 mm apical to the bracket slot with the ARH 5 to 6 mm apical to the bracket slot. With this assembly, the force would pass just under the CoR and induce nearly bodily retraction with only slight lingual tipping and intrusion.19
The present study, however, measured only the initial displacement and the stresses generated immediately after force application. As the teeth move, a counter-moment would be generated in the bracket slot, thus when forces act for a longer period of time; different results may be obtained clinically. Also, PDL and alveolar bone were assumed to be isotropic and homogeneous to simplify the interpretation of the study. The results of this study were based on a single CT scan model and cannot be extrapolated in all clinical situations as such, because the pattern of bone loss may vary in different individuals. Nevertheless, the study provides a brief perspective of the effect of bone loss on mini-implant-anchored en- masse retraction.
CONCLUSION
In order to minimize the tipping and the stress in the PDL, the height of ARH should be increased even further in alveolar bone loss conditions to allow retraction force to pass through or even further above the CoR of anterior teeth, though this may not be clinically suitable due to chances of irritation to the vestibular mucosa.
CLINICAL SIGNIFICANCE
An alternative is to apply a lighter retraction force to reduce the lingual tipping moment.A higher counter-moment in the archwire or in the bracket can also be incorporated which poses more strain on the anchorage unit. But with the advent of mini-implant, direct or indirect anchorage can be obtained without affecting the posterior teeth.
REFERENCES
1. Artun J, Urbye K. The effect of orthodontic treatment on periodontal bone support in patients with advanced loss of marginal periodontium. Am J Orthod Dentofac Orthop 1988;93(2):143–148. DOI: 10.1016/0889-5406(88)90292-2.
2. Boyd RL, Leggott PJ, Quinn RS, et al. Periodontal implications of orthodontic treatment in adults with reduced or normal periodontal tissues versus those of adolescents. Am J Orthod Dentofac Orthop 1989;96(3):191–199. DOI: 10.1016/0889-5406(89)90455-1.
3. Melsen B, Agerbaek N, Markenstam G. Intrusion of incisors in adult patients with marginal bone loss. Am J Orthod Dentofac Orthop 1989;96(3):232–241. DOI: 10.1016/0889-5406(89)90460-5.
4. Yoshida N, Koga Y, Mimaki N, et al. In vivo determination of the centres of resistance of maxillary anterior teeth subjected to retraction forces. Eur J Orthod 2001;23(5):529–534. DOI: 10.1093/ejo/23.5.529.
5. Geramy A. Alveolar bone resorption and the center of resistance modification (3-D analysis by means of the finite element method). Am J Orthod Dentofac Orthop 2000;117(4):399–405. DOI: 10.1016/s0889-5406(00)70159-4.
6. Padmawar SS, Belludi A, Makhija PG, et al. Stress appraisal with simulation of en masse absolute intrusion of maxillary anteriors deploying strategic mini-implant locations: a finite element analysis. J Indian Orthod Soc 2012;46:77–81. DOI: 10.5005/jp-journals-10021-1064.
7. Tominaga JY, Tanaka M, Koga Y, et al. Optimal loading conditions for controlled movement of anterior teeth in sliding mechanics: a 3D finite element study. Angle orthod 2009;79(6):1102–1107. DOI: 10.2319/111608-587R.1.
8. Smith RJ, Burstone CJ. Mechanics of tooth movement. Am J Orthod 1984;85(4):294–307. DOI: 10.1016/0002-9416(84)90187-8.
9. Geramy A. Initial stress produced in the periodontal membrane by orthodontic loads in the presence of varying loss of alveolar bone: a three‐dimensional finite element analysis. Eur J Orthod 2002;24(1):21–33. DOI: 10.1093/ejo/24.1.21.
10. Tanne K, Nagataki T, Inoue Y, et al. Patterns of initial tooth displacements associated with various root lengths and alveolar bone heights. Am J Orthod Dentofac Orthop 1991;100(1):66–71. DOI: 10.1016/0889-5406(91)70051-W.
11. Cobo J, Sicilia A, Argüelles J, et al. Initial stress induced in periodontal tissue with diverse degrees of bone loss by an orthodontic force: tridimensional analysis by means of the finite element method. Am J Orthod Dentofac Orthop 1993;104(5):448–454. DOI: 10.1016/0889-5406(93)70071-U.
12. Cobo J, Argfielles J, Puente M. Dentoalveolar stress from bodily tooth movement at different levels of bone loss. Am J Orthod Dentofac Orthop 1996;110(3):256–262. DOI: 10.1016/s0889-5406(96)80008-4.
13. Jeon PD, Turley PK, Ting K. Three-dimensional finite element analysis of stress in the periodontal ligament of the maxillary first molar with simulated bone loss. Am J Orthod Dentofacial Orthop 2001;119(5):498–504. DOI: 10.1067/mod.2001.112999.
14. Ona M, Wakabayashi N. Influence of alveolar support on stress in periodontal structures. J Dent Res 2006;85(12):1087–1091. DOI: 10.1177/154405910608501204.
15. Sung SJ, Jang GW, Chun YS, et al. Effective en-masse retraction design with orthodontic mini implant anchorage: a finite element study. Am J Orthod Dentofac Orthop 2010;137(5):648–657. DOI: 10.1016/j.ajodo.2008.06.036.
16. Ammar HH, Ngan P, Crout RJ, et al. Three-dimensional modeling and finite element analysis in treatment planning for orthodontic tooth movement. Am J Orthod Dentofac Orthop 2011;139(1):e59–e71. DOI: 10.1016/j.ajodo.2010.09.020.
17. Nanda R, Ghosh J. Biomechanical considerations in sliding mechanics. In: Nanda R, editor. Biomechanics in clinical orthodontics. Philadelphia: W. B. Saunders; 1997. p. 188–217.
18. Sia S, Shibazaki T, Koga Y, et al. Experimental determination of optimal force system required for control of anterior tooth movement in sliding mechanics. Am J Orthod Dentofac Orthop 2009;135(1):36–41. DOI: 10.1016/j.ajodo.2007.01.034.
19. Park HS, Kwon TG. Sliding mechanics with microscrew implant anchorage. Angle Orthod 2004;74(5):703–710. DOI: 10.1043/0003-3219(2004)074<0703:SMWMIA>2.0.CO;2.
________________________
© The Author(s). 2021 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.