ORIGINAL RESEARCH |
https://doi.org/10.5005/jp-journals-10024-3224 |
Effectiveness of Pre-administered Natural Sweet-tasting Solution for Decreasing Pain Associated with Dental Injections in Children: A Split-mouth Randomized Controlled Trial
1,2Department of Paediatric and Preventive Dentistry, Saveetha Dental College and Hospital, Saveetha Institute of Medical and Technical Science, Saveetha University, Chennai, Tamil Nadu, India
Corresponding Author: Palak Janiani, Department of Paediatric and Preventive Dentistry, Saveetha Dental College and Hospital, Saveetha Institute of Medical and Technical Science, Saveetha University, Chennai, Tamil Nadu, India, Phone: +91 9820775554, e-mail: palakjaniani@gmail.com
How to cite this article: Janiani P, Gurunathan D. Effectiveness of Pre-administered Natural Sweet-tasting Solution for Decreasing Pain Associated with Dental Injections in Children: A Split-mouth Randomized Controlled Trial. J Contemp Dent Pract 2021;22(12):1434–1437.
Source of support: Nil
Conflict of interest: None
ABSTRACT
Aim: This study aimed to discern if a prior intake of a natural sweet remedy (honey) impacted pain perception during intraoral injections.
Materials and methods: One hundred healthy children who needed the same treatment bilaterally in either arch which required local anesthetic administration (infiltration in maxillary arch and inferior alveolar nerve block in mandibular arch) were recruited. The patients’ demographic details were recorded. Local anesthesia was administered after taking 5 mL of honey solution on the test side and 5 mL of sterile water on the control side. Subjective pain perception during injection was measured using Wong–Baker Faces Pain Rating Scale and objective pain by sound, eye, body movement (SEM) rating scale. The parametric data were analyzed using a paired Student’s t-test (p <0.05). Level of consensus between the two scales was assessed using Pearson’s correlation.
Results: The test side yielded lower mean Wong–Baker Faces Pain Rating Scale (3.72 ± 1.80) and SEM (4.12 ± 1.04) scores than the control side (6.00 ± 2.06 and 5.00 ± 1.45 respectively). This was statistically significant.
Conclusion: The administering of a natural sweet solution such as honey before dental injections in children tends to reduce the discomfort and pain associated with the procedure.
Clinical significance: Pain management is of utmost importance in dentistry, especially among children. The consumption of natural foods such as honey helps in decreasing injection pain perception, making the child cooperative, and thereby allowing the dentist to provide the best dental care.
Keywords: Honey, Injection, Local anesthesia, Pain.
INTRODUCTION
The administration of local anesthetics is one of the most dreaded or anxiety-inducing triggers in a dental setup.1,2 Patients, particularly children, may be fearful of dental injections, which may prevent them from seeking dental treatment. Even though profound local anesthesia aids in the treatment of pediatric patients in terms of reducing their anxiety and pain during restorative and surgical procedures,3 the fear of needles has been cited as a barrier to developing proper dental care.4,5
Numerous techniques have been researched in an attempt to minimize the pain and distress associated with these dental injections, varying from localized methods to distraction techniques. The localized methods include application of topical agents,6 altering the rate of injection, pre-cooling the site, increasing the pH of local anesthetics by buffering7 and pretreatment with lasers.8 Instruments such as WAND System (Wand Dental, Inc., Livingston, New Jersey, USA),9 and DentalVibe are also available to make dental injections more comfortable.
In clinical settings, the use of orally administered sweet-tasting solutions for neonatal pain relief is popular and recommended in guidelines given nationally and internationally.
Studies have found that sweet-flavored solutions, mainly 30% sucrose, given orally prior to cutaneous procedures can reduce discomfort in neonates undergoing heel sticks and venipuncture.10–12 Effectiveness of sucrose in the treatment of procedural pain in newborns and babies has been verified in a Cochrane review by Harrison et al.12
The analgesic activity of sweet compounds in young children has been reported by very few studies.12–14 Of these, two trials have investigated the impact of sweet formulations on analgesia for treatments involving needle injections. According to Harrison et al., there is insufficient evidence of the sweet taste acting as an analgesic in reducing pain associated with needle pricks in infants.12,15 Lewkowski et al. reported sweet-tasting chewing gums to be ineffective in treating pain caused by injections.13 However, in comparison, all of the experiments that studied the impact of sucrose on cold pressor test (CPT), a tool for determining pain threshold, found that the analgesic effect was mild in children.15,16
Due to the commonly experienced severe and pervasive anxiety as a result of injections in the dental sector, any method or system that can help with anxiety or pain relief should be considered. Considering that few studies have demonstrated sweet-tasting solutions to have a mild analgesic activity in infants, the purpose of this study is to see whether the prior consumption of a natural sweet solution such as honey affects the pain perceived by children after dental injections.
MATERIALS AND METHODS
This randomized controlled trial, having a split-mouth design, was carried out after getting approval from the Institutional Review Board and Ethics Committee (IHEC/SDC/PEDO-2001/21/30) at a dental university setting in Chennai, India. One hundred children who reported to the Department of Paediatric and Preventive Dentistry needing the same treatment bilaterally in either arch, which necessitated local anesthetic administration, were recruited. Uncooperative children (Frankl rating #1 or #2), those with an allergy to lignocaine or honey and with a history of abscess or fistula in the injection site, were excluded.
Children who met the inclusion criteria were randomly recruited from October 2020 to March 2021 by an investigator who was unaware of the study protocol, excluding the eligibility criteria. Seventy-two children were finally included. Each patient’s parents/legal guardians provided written informed consent for participation and publishing in compliance with the Declaration of Helsinki’s ethical criteria. On the first appointment, a coin toss was carried out to decide which side would be the control and test group. This was carried out by the same investigator. The participants were asked to drink 5 mL of honey solution before injecting on the experimental side, while the control side got 5 mL of sterile water in the same way. For both solutions, the patient was asked to hold the solution in the mouth for a minute and then to spit it out. Two different treatment sessions, with an interval of seven days, were carried out for this study: one for the experimental side and one for the control side. A CONSORT flow diagram depicts the recruiting and distribution of the sample population (Flowchart 1).

Flowchart 1: CONSORT flowchart indicating allocation of participants in each group
The side which would be treated first was decided based on the patient’s chief complaint. A pediatric dentist who was unaware about the solution that was given to the patient administered all local anesthetic injections (inferior alveolar and lingual nerve blocks or buccal infiltration). Both injections used 2% lidocaine with 1:100,000 epinephrine, and a 27-gauge needle. At each appointment, only one single tube of anesthetic was used (1.8 mL) for the injection, after which the pain perceived was recorded using Wong–Baker Faces Pain Rating Scale and sound, eye, body movement (SEM) rating scale. Before the injection, the patients were instructed on how to rate their pain using the Wong–Baker Faces Pain Rating Scale. SEM scores range from 0 to 9 based on 0–3 scores for every parameter. If any discomfort was experienced during the treatment procedure, after recording the Wong–Baker Faces Pain Rating Scale and SEM, a supplementary infiltration injection was given to ensure full anesthesia.
The data collected were tabulated and analyzed by SPSS software version 20.0 (SPSS Inc, Chicago, Illinois). Paired Student’s t-test was carried out for the analysis of the parametric data, for which the statistical significance was defined at p <0.05. Pearson’s correlation was done too to assess the level of consensus between the objective and subjective scales used (p <0.001).
RESULTS
Two categories were formed of the 72 participants, having a mean age of 9 ± 3.9 years, depending on which solution was given first, with 32 people having the control (sterile water) and the other 40 getting the honey solution first. Table 1 shows the demographic statistics for the participants.
| Frequency | ||
|---|---|---|
| Age (year ± SD ) | 9 ± 3.9 years | |
| Gender | F | 20 (27.8%) |
| M | 52 (72.2%) | |
| Type of injection | IAN | 44 (61.1%) |
| Maxillary infiltration | 28 (38.9%) |
The study reveals that prior treatment of a sweet solution (3.7 ± 1.81) resulted in a substantially lower mean Wong–Baker Faces Pain Rating Scale score than the test side (6.0 ± 2.06) (p <0.05). Statistical research revealed that as compared to the control group, sweet taste resulted in a slightly lower, yet significant, reduction in mean SEM (p <0.05) (Table 2).
| Mean ± SD | p value | ||
|---|---|---|---|
| Wong–Baker Faces Pain Rating Scale | Water | 6.0 ± 2.06 | 0.000* |
| Honey | 3.7 ± 1.81 | ||
| SEM rating | Water | 5.00 ± 1.46 | 0.007* |
| Honey | 4.17 ± 1.04 |
Figures 1 and 2 show the pain levels on the Wong–Baker Faces Pain Rating Scale and SEM scale, respectively, for each anesthetic technique after the administration of the solutions. It is seen that on both scales, the pain values after intake of honey solution are lower than the control solution. This is applicable for both techniques: inferior alveolar nerve block as well as maxillary infiltration.
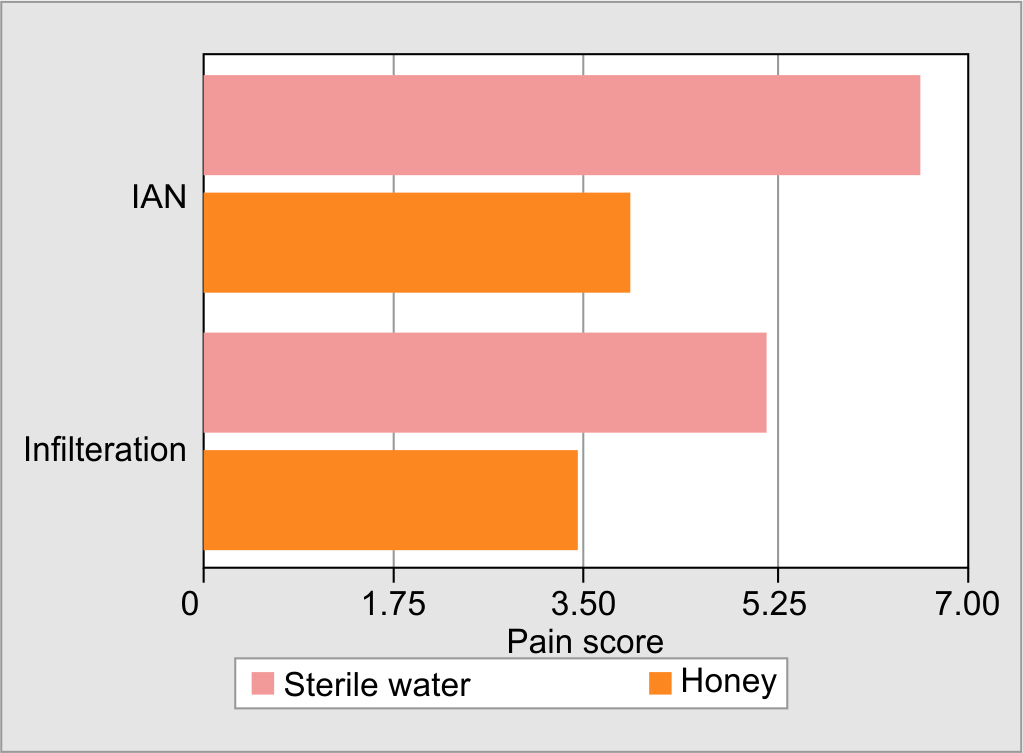
Fig. 1: Bar graph representing the mean values obtained in Wong–Baker Faces Pain Rating Scale for each anesthetic technique after administration of sterile water
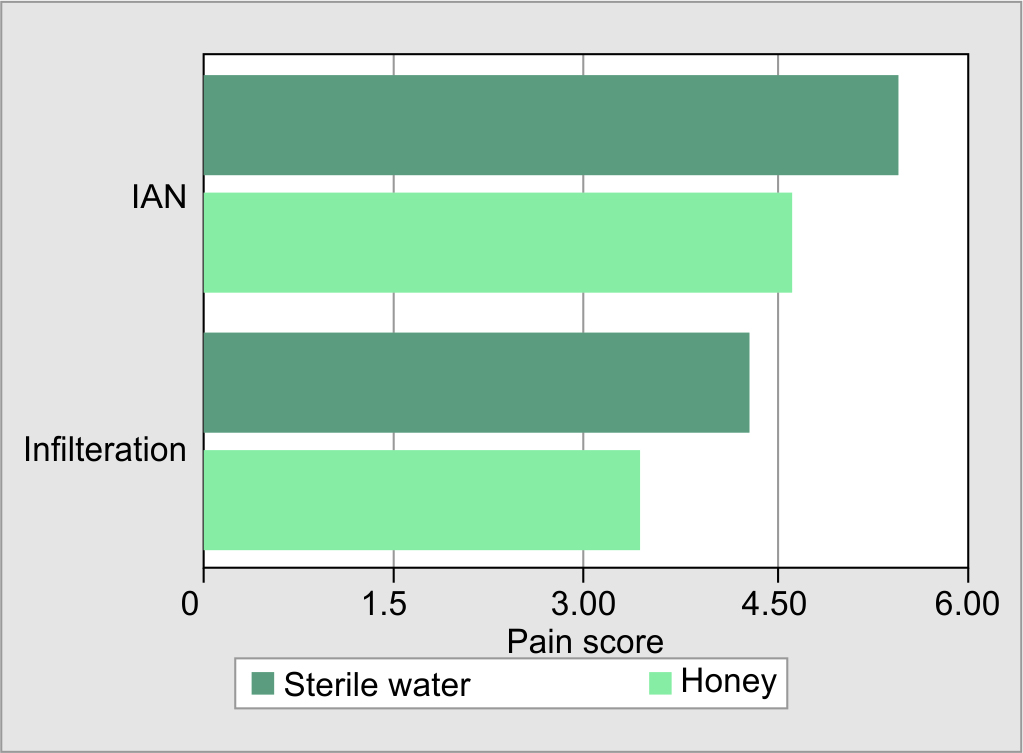
Fig. 2: Bar graph representing the mean values obtained in SEM scale for each anesthetic technique after administration of sterile water and honey solution
According to Pearson’s correlation coefficient, there was a strong level of consensus between Wong–Baker Faces Pain Rating Scale and SEM measurements of pain decrement (r = 0.786; p <0.001).
DISCUSSION
From routine pediatric immunizations to dental treatment, children across all ages are subject to traumatic needle-associated treatments. Although necessary, these procedures are considered to be uncomfortable, causing discomfort and apprehension in both children and their parents, as well as the possibility of developing long-term fears of needle pain.17 Therefore, efficient pain relief techniques must be used routinely in all areas, where needle-related operations are performed to alleviate this fear. This study aimed to see how tasting a sweet solution affected the pain caused by a dental injection. The discomfort and pain associated with the injections were seen to be lesser when children were given a sweet-tasting honey solution.
For the last century, and well before that, oral sucrose and other sweet remedies have been used to relieve discomfort in children. From the 1840s to the early 1900s, a date and sugar solutions laced with alcohol, cocaine, or opium were recommended for infants for the same.18 Even though the use of sucrose solution has been advocated and extensively studied on,9,10 our study used honey as it has an antibacterial activity on S. mutans which can reduce dental caries.19 Honey is a naturally derived sweetener which is a healthier option than sucrose, which is cariogenic.
In our study, the objective pain recorded by Wong–Baker Faces Pain Rating Scale showed a greater overall reduction in pain than the SEM scale showed (Figs 1 and 2, respectively). This could be attributed to the immature descending control systems in young children making them unable to comprehend abstract ideas due to which it may be difficult for them to differentiate the level of pain. Children are most likely to choose the extremes of pain scales, ignoring the middle scores or multiple-item scales.20Adolescents, on the contrary, appear to suppress pain manifestations for fear of discomfort, which can result in lower registered pain levels.21 For a more precise measure of children’s pain perception, two scales were used: the Wong–Baker Faces Pain Rating Scale, a nonverbal instrument with illustrations, and SEM, a subjective analytical tool.
Lewkowski et al. conducted a study where a sweet-tasting chewing gum was given before an injection. However, as opposed to our study’s results, they found that it did not relieve discomfort associated with the needle prick. This discrepancy may be attributed to the means by which the sweet material was administered. The control group in the same study also got gum, and it was proposed that the rhythmic activity involved in chewing could induce analgesia, masking the sweet taste effect.13 Furthermore, sweet compounds released from a gum do not have the same potency as honey solution kept in the mouth, which was the approach used in this research.
The specific mechanism by which sweet taste decreases pain is an area where further study is required. An increase in the endogenous opioid production was seen in response to the administration of sweet substances in many studies. Using function magnetic resonance imaging (fMRI), Kakeda et al.22 showed that keeping a sweet-tasting solution in the mouth resulted in a positive affective state. This heightened affective status has been found to have the ability to suppress the sense of pain. Analgesia is caused only when the sweet material is put on the tongue, not when it is given through a nasogastric conduit. This supports the theory that the sugar, and not the sweet taste, has pain-relieving properties. According to this theory, perception of taste can play a role in the outcomes seen, implying that a decreased capacity to sense a sweet flavor can lead to less analgesia. The participants in this study were not tested priorly to assess their capacity for detecting a sweet flavor, which could have led to less analgesia. Another limitation of this study would be the small sample size.
CONCLUSION
Honey solution was shown to be effective in mitigating the discomfort induced by dental injections; pain associated with both infiltration and inferior alveolar nerve block was decreased after the intake. Although there are many ways to control discomfort in the age-group studied, using a natural sweet solution has the advantage of being entirely healthy and providing the user with a good experience, with the sweet taste being an additional benefit.
Clinical Significance
Pain caused by dental injections is widely feared, more so among children. The use of a natural sweetener such as honey could be incorporated on a regular basis before injecting intraorally, due to its ability to reduce the discomfort induced by dental injections, noncariogenic property, and easy acceptance by the patients.
Authors’ Contributions
PJ and DG conceived the ideas; PJ collected and analyzed the data; and PJ and DG led the writing.
REFERENCES
1. Bedi R, Sutcliffe P, Donnan PT, et al. The prevalence of dental anxiety in a group of 13- and 14-year-old Scottish children. Int J Paediatr Dent 1992;2(1):17–24. DOI: 10.1111/j.1365-263x.1992.tb00003.x.
2. Dahlander A, Soares F, Grindefjord M, et al. Factors associated with dental fear and anxiety in children aged 7 to 9 years. Dent J (Basel) 2019;7(3):68. DOI: 10.3390/dj7030068.
3. Nowak A, Christensen JR, Mabry TR, et al. In: Pediatric dentistry— E-Book: infancy through adolescence. 6th ed. Elsevier Health Sciences; 2018. 656 p.
4. Milgrom P, Coldwell SE, Getz T, et al. Four dimensions of fear of dental injections. J Am Dent Assoc 1997;128(6):756–766. DOI: 10.14219/jada.archive.1997.0301.
5. McDonald RE, Avery DR, Dean JA, et al. Local anesthesia and pain control for the child and adolescent. In: McDonald RE, Avery DR, Dean JA, editors. Dentistry for the child and adolescent. 9th ed. St Louis, MO: CV Mosby Inc.; 2011. p. 241–252.
6. O’Brien L, Taddio A, Lyszkiewicz DA, et al. A critical review of the topical local anesthetic amethocaine (Ametop) for pediatric pain. Paediatr Drugs 2005;7(1):41–54. DOI: 10.2165/00148581-200507010-00004.
7. Younis I, Bhutiani RP. Taking the ‘ouch’ out–effect of buffering commercial xylocaine on infiltration and procedure pain–a prospective, randomised, double-blind, controlled trial. Ann R Coll Surg Engl 2004;86(3):213–217. DOI: 10.1308/003588404323043382.
8. Ghaderi F, Ghaderi R, Davarmanesh M, et al. Pain management during needle insertion with low level laser. Eur J Paediatr Dent 2016;17(2):151–154. PMID: 27377115.
9. Tung J, Carillo C, Udin R, et al. Clinical performance of the DentalVibe® injection system on pain perception during local anesthesia in children. J Dent Child (Chic) 2018;85(2):51–57. PMID: 30345954.
10. Stevens B, Yamada J, Lee GY, et al. Sucrose for analgesia in newborn infants undergoing painful procedures. Cochrane Database Syst Rev 2013;(1):CD001069. DOI: 10.1002/14651858.CD001069.pub4.
11. Ventura AK, Mennella JA. Innate and learned preferences for sweet taste during childhood. Curr Opin Clin Nutr Metab Care 2011;14(4):379–384. DOI: 10.1097/MCO.0b013e328346df65.
12. Harrison D, Stevens B, Bueno M, et al. Efficacy of sweet solutions for analgesia in infants between 1 and 12 months of age: a systematic review. Arch Dis Child 2010;95(6):406–413. DOI: 10.1136/adc.2009.174227.
13. Lewkowski MD, Barr RG, Sherrard A, et al. Effects of chewing gum on responses to routine painful procedures in children. Physiol Behav 2003;79(2):257–265. DOI: 10.1016/s0031-9384(03)00098-2.
14. Pepino YM, Mennella JA. Sucrose-induced analgesia is related to sweet preferences in children but not adults. Pain 2005;119(1–3):210–218. DOI: 10.1016/j.pain.2005.09.029.
15. Harrison D, Yamada J, Adams-Webber T, et al. Sweet tasting solutions for reduction of needle-related procedural pain in children aged one to 16 years. Cochrane Database Syst Rev 2015;2015(5):CD008408. DOI: 10.1002/14651858.CD008408.pub3.
16. Miller A, Barr RG, Young SN. The cold pressor test in children: methodological aspects and the analgesic effect of intraoral sucrose. Pain 1994;56(2):175–183. DOI: 10.1016/0304-3959(94)90092-2.
17. Diekema DS. Improving childhood vaccination rates. N Engl J Med 2012;366(5):391–393. DOI: 10.1056/NEJMp1113008.
18. Bean WB. The golden age of quackery. Journal of the American Medical Association 1960;174(10):1351–1352. DOI: 10.1001/jama.1960.03030100119040.
19. Ahmadi-Motamayel F, Hendi SS, Alikhani MY, et al. Antibacterial activity of honey on cariogenic bacteria. J Dent (Tehran) 2013;10(1):10–15. PMID: 23724198.
20. Smolarek PC, da Silva LS, Martins PRD, et al. Evaluation of pain, disruptive behaviour and anxiety in children aging 5-8 years old undergoing different modalities of local anaesthetic injection for dental treatment: a randomised clinical trial. Acta Odontol Scand 2020;78(6):445–453. DOI: 10.1080/00016357.2020.1757752.
21. Franck LS, Greenberg CS, Stevens B. Pain assessment in infants and children. Pediatr Clin North Am 2000;47(3):487–512. DOI: 10.1016/s0031-3955(05)70222-4.
22. Kakeda T, Ogino Y, Moriya F, et al. Sweet taste-induced analgesia: an fMRI study. Neuroreport 2010;21(6):427–431. DOI: 10.1097/WNR.0b013e3283383df5.
________________________
© The Author(s). 2021 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.